

Concomitant Atrial Fibrillation Ablation and Left Atrial Appendage Occlusion in Aging Patients With Atrial Fibrillation: Experience at the Cardiovascular Institute of Scottsdale
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2026;26(4):18-19.
Ashish Sadhu, MD, FHRS, FACC
The electrophysiology (EP) program at the Cardiovascular Institute of Scottsdale has refined a concomitant strategy for the treatment of atrial fibrillation (AF) that combines pulmonary vein isolation (PVI), with or without additional non-pulmonary vein ablation using pulsed field ablation (PFA) (Farapulse, Boston Scientific), and left atrial appendage occlusion (LAAO). The procedure is guided by 4-dimensional (4D) intracardiac echocardiography (ICE) and supported by integrated mapping (Opal HDx Mapping System, Boston Scientific). This approach is designed for older patients with elevated CHA₂DS₂-VASc scores and increased bleeding risk who may be candidates for a single procedural alternative to long-term oral anticoagulation. This combined approach may provide rhythm control and stroke risk reduction in a single procedure, potentially minimizing repeat anesthesia exposure and procedural burden in appropriately selected patients. The aim of this article is to describe the procedural workflow, patient selection criteria, and clinical rationale for a combined approach integrating PFA, 3-dimensional (3D) electroanatomic mapping, and 4D ICE with LAAO for the treatment of AF in older patients at increased risk for bleeding.
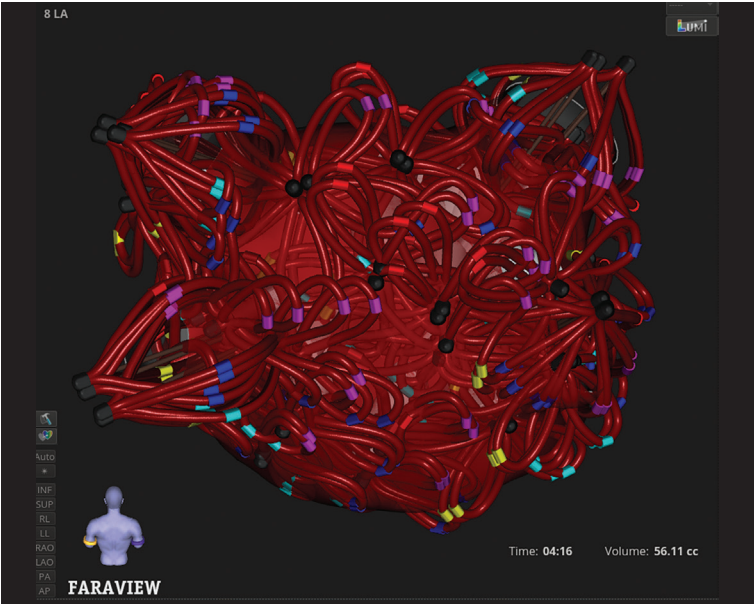
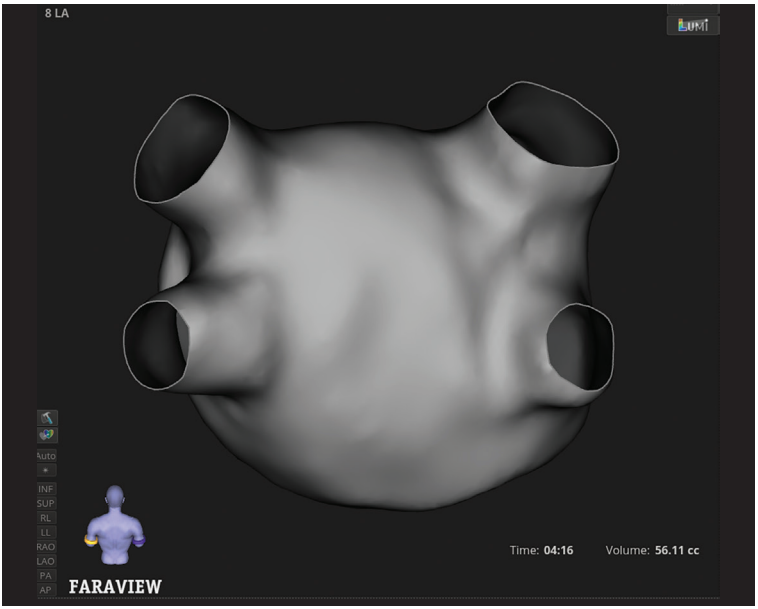
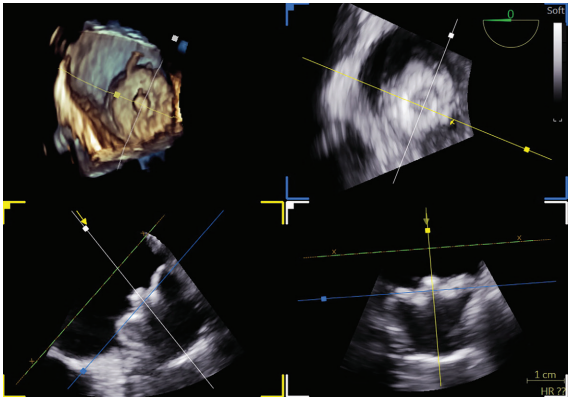
Use of 4D ICE enables real-time visualization of the left atrium (LA) and LAA, eliminating the need for transesophageal echocardiography (TEE). The spatial resolution and volumetric imaging provided by 4D ICE facilitate both phases of the combined procedure by confirming catheter contact during PFA and guiding accurate device deployment during LAAO. Integration with electroanatomical mapping allows for detailed reconstruction of the LA and PVs, supporting precise lesion delivery and confirmation of durable isolation during PFA.
PFA offers a nonthermal method of energy delivery that selectively ablates myocardial tissue while sparing adjacent structures. This mechanism may be particularly beneficial in older patients, in whom esophageal protection and phrenic nerve function are important considerations. When used in conjunction with 3D electroanatomical mapping, PFA allows accurate lesion placement with minimal collateral injury, providing an appropriate balance in patients with age-related frailty and comorbid conditions.
The integration of PFA, 3D mapping, and 4D ICE has established a procedural workflow designed to improve safety, comfort, and efficiency in older patients. This combined approach—leveraging novel energy sources, advanced imaging, and streamlined logistics—allows for arrhythmia management and stroke prevention within a single procedure, reflecting an evolving model of care in cardiac EP.
The OPTION randomized trial provided key data supporting the safety of combining AF ablation with LAAO.1 Among 654 patients who underwent concomitant procedures, those randomized to the device group experienced outcomes noninferior to those of patients receiving oral anticoagulation for the composite endpoint of death, stroke, and systemic embolism at 36 months. The primary safety endpoint—nonprocedural major or clinically relevant nonmajor bleeding—occurred significantly less often in the device group (8.5% vs 18.1%; P<.001). Acute procedural complication rates were similar between groups, indicating that the addition of LAAO to AF ablation did not increase immediate procedural risk.2 These findings suggest that combining rhythm control and stroke prevention within a single procedure may be particularly beneficial in older patients, in whom procedural morbidity and long-term bleeding risk are important considerations.
Sample Case
A 75-year-old woman with a CHA₂DS₂-VASc score of 5 presented with dilated cardiomyopathy, a history of biventricular implantable cardioverter-defibrillator placement, and symptomatic persistent drug-refractory AF. The patient experienced a gastrointestinal hemorrhage that required hospitalization and packed red blood cell transfusions on 2 occasions.
Intraprocedural imaging and mapping were performed using 4D ICE via a 11 French venous sheath and 3D electroanatomic mapping to guide transseptal access, verify lesion delivery, and confirm optimal LAA device position, all under conscious sedation. The 4D ICE provided volumetric, high-resolution visualization of the LA and LAA in real time, while 3D mapping allowed detailed electroanatomic reconstruction and accurate lesion targeting with reduced reliance on fluoroscopy.
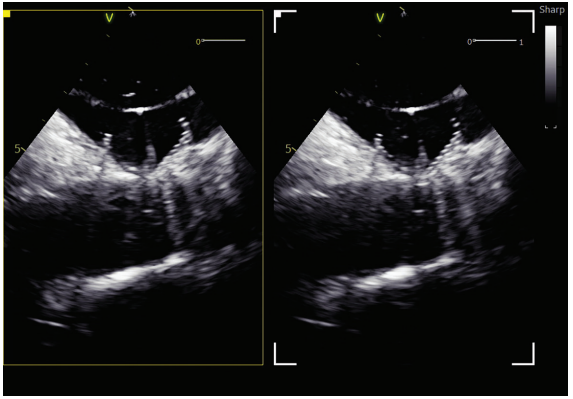
A transseptal catheterization was performed using the Faradrive Steerable Sheath (Boston Scientific) and Faraconnect dilator, along with VersaCross Access Solution (Boston Scientific), in the low to mid septum and slightly anterior position to facilitate the ablation and subsequent exchange for the Watchman TruSteer (Boston Scientific) delivery sheath for an optimal ablate-and-close procedure. LAA measurements obtained before ablation were 18 to 19 mm in 3 views (short-axis/mid LA, long-axis, and supramitral). No significant edematous change was observed in the limbus after ablation. A 27-mm Watchman FLX Pro LAAO device was selected, which completely sealed the LAA without residual leak on color flow imaging. Postdeployment measurements were 19 to 20 mm in 3 ICE views, including multiplanar reconstruction using the 4D ICE Nuvision Ultrasound Catheter (Johnson & Johnson MedTech). The patient tolerated the procedure without complications.
PFA was used as a nonthermal, tissue-selective ablation modality designed to limit collateral injury to adjacent structures such as the esophagus and phrenic nerve—critical when treating frail, aging myocardium. Preclinical and early clinical data have suggested that PFA may produce more uniform lesions and fewer complications than thermal ablation techniques.
Summary
At the Cardiovascular Institute of Scottsdale, a concomitant strategy has been implemented for selected older patients with AF. The combined approach consolidates atrial ablation and LAAO into a single procedure. Postprocedural evaluation includes follow-up imaging with computed tomography or TEE and continued management in a dedicated AF clinic.
Disclosures: Dr Sadhu has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. He has no conflicts of interest to report.
References
- Wazni OM, Saliba W, Nair DG, et al. Left atrial appendage closure after ablation for atrial fibrillation. N Engl J Med. 2025;392(13):1277-1287. doi:10.1056/NEJMoa2408308
- Saliba W, Nair D, Swarup V, et al. Comparison of left atrial appendage closure and oral anti-coagulation after catheter ablation for atrial fibrillation: concomitant and sequential cohorts of the OPTION randomized controlled trial. Heart Rhythm. 2025;22(10):2585-2594. doi:10.1016/j.hrthm.2025.04.029

