When to Fix, and When Not to Fix, Ankle Fractures: Evidence-Based Decision Making for the Foot and Ankle Surgeon
Ankle fracture management is increasingly guided by mortise stability and patient factors, not simply fracture pattern or the number of malleoli involved. Even subtle talar malalignment can dramatically alter tibiotalar contact mechanics and accelerate post-traumatic arthritis, making accurate assessment of congruency essential. This article offers a practical, evidence-based framework to help foot and ankle surgeons decide when fixation is warranted, and when nonoperative care is the better choice.
Key Takeaways
1. Stability—not classification—drives treatment decisions. Any fracture demonstrating talar shift/tilt, medial clear space widening, syndesmotic disruption, or inability to maintain congruent mortise alignment should be considered unstable and generally treated operatively if the patient can tolerate surgery.
2. Weight-bearing radiographs better reflect functional instability than stress views in select cases. In isolated Weber B fractures, stress radiographs may overestimate instability, while weight-bearing imaging can more reliably identify patients who can do well with nonoperative management; provided close follow-up confirms sustained alignment.
3. Nonoperative management is an active plan, especially for high-risk patients. Stable mortise alignment, medical frailty, poor soft-tissue/vascular status, or elevated wound complication risk may tip the balance toward casting/functional treatment—with early reassessment and serial imaging to catch any loss of reduction that would require timely conversion to surgery.
Ankle fractures are among the most common injuries encountered in a foot and ankle practice, yet the correct treatment is not dictated by fracture pattern in isolation. The current decision point of consideration is to determine the stability of the ankle mortise (and the patient’s ability to tolerate surgery), not simply the fracture pattern or number of malleoli involved. Even though persistent controversy exists regarding operative indications of ankle fractures, the goal remains consistent: restore and maintain a congruent tibiotalar joint. A classic biomechanical study, confirmed by another cadaveric study, demonstrates the first 1 mm of lateral talar shift reduced tibiotalar contact area by an average of 42%, supporting why even subtle mortise malalignment matters clinically to prevent abnormal joint loading and accelerated cartilage degeneration.1,2 Thus, any ankle fracture where the talus translates or tilts within the mortise under load should be considered unstable, and generally treated operatively, unless patient-specific risks outweigh the benefits of surgical intervention. This foundational concept frames current ankle fracture management.
This article aims to provide a literature-based practical framework to assist in determining when operative fixation is indicated, or when nonoperative management is more appropriate.
Determining Stability: Radiographic and Functional Assessment
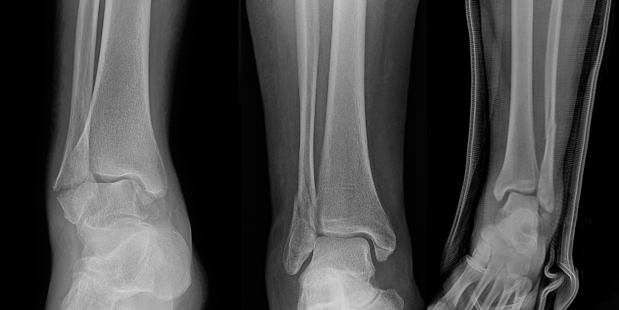
Standard Radiographs. Initial evaluation includes standard anteroposterior, lateral, and mortise radiographic views. Important findings to suggest tibiotalar joint instability include: talar shift or tilt, widened medial clear space (>4 mm or asymmetry compared with the contralateral clear space), fibular shortening or malrotation, and posterior malleolar displacement affecting joint congruency (Figure 1).

Stress Radiographs. Gravity or external rotation stress radiographs traditionally assess deltoid ligament integrity, particularly in isolated Weber B fractures. However, multiple studies demonstrate stress radiographs may overestimate instability, which may identify partial deltoid injuries that do not translate into functional ankle instability (Figure 2).3-5
Weight-Bearing Radiographs. More recent literature supports weight-bearing radiographs as a reliable and clinically relevant method to assess functional stability in select ankle fractures, particularly isolated Weber B injuries. Prospective studies show that patients with stable weight-bearing mortise alignment experience excellent outcomes with nonoperative treatment, even when stress views suggest instability.4-8 Although, a recent study by Zonneveld and Hoogendoorn in 2024 found substantial variability in the amount of weight-bearing on an ankle during weight-bearing radiographs, and to keep this information in mind when determining a treatment course.9
When to Fix Ankle Fractures
1. Any Fracture with an Incongruent Mortise
Persistent talar displacement, either at presentation or following attempted reduction, is a strong indication for operative fixation. Even minimal residual talar malalignment can significantly alter tibiotalar contact mechanics, resulting in increased focal contact pressures and accelerated cartilage degeneration.1 As previously mentioned, failure to restore anatomic congruity is therefore associated with inferior functional outcomes and a substantially increased risk of post-traumatic ankle arthritis, as classically demonstrated by Ramsey and Hamilton and supported by subsequent clinical outcome studies.1,2,10 Additional indications include lateral talar shift, progressive displacement on serial radiographs during nonoperative care, and an inability to maintain reduction with closed means.
2. Unstable Fracture Patterns
While fracture classification alone should not dictate treatment, certain injury patterns are consistently associated with mechanical instability and therefore more frequently require operative fixation. Displaced bimalleolar and trimalleolar fractures, Weber C and Maisonneuve injuries, fracture-dislocations, open fractures or fractures with significant soft tissue compromise reliably demonstrate disruption of the ankle mortise and loss of tibiotalar congruity. These patterns often reflect high energy and/or rotational mechanisms and are commonly accompanied by syndesmotic injury, deltoid ligament incompetence, or posterior malleolar involvement, all of which contribute to persistent instability if left unaddressed. The Lauge-Hansen classification highlights these predictable associations between mechanism of injury and ligamentous and osseous failure, reinforcing the importance of restoring both anatomic alignment and mortise stability to optimize functional outcomes and reduce the risk of post-traumatic arthritis.11

3. Syndesmotic Instability
Syndesmotic injury is a key driver of ankle instability. Clinical examination, radiographic parameters (ie, decreased tibia-fibula overlap), and a thorough intraoperative assessment guide the need for stabilization. There are various ways to stress the syndesmosis including the hook test, which has been shown to be somewhat unreliable in determining syndesmotic instability.12 Arthroscopic evaluation of the syndesmosis provides a reliable evaluation of the syndesmosis.13 However the method of testing the integrity of the syndesmosis, it is important to highlight the necessity of fixation when indicated, as shown by Pogliacomi and colleagues in 2021.14 Meta-analyses of randomized trials show suture-button fixation provides equivalent or improved functional outcomes with lower reoperation rates compared with syndesmotic screws, particularly by avoiding routine hardware removal.15-17 Syndesmotic instability is a critical determinant of ankle fracture stability, requiring careful clinical, radiographic, and sometimes arthroscopic assessment to guide fixation (Figure 3).

4. Posterior Malleolus Fractures Affecting Stability
Traditional fixation thresholds based solely on fragment size (>25–30% of articular surface) have been challenged. Current evidence suggests fixation should be considered when the posterior malleolar fragment contributes to articular incongruity or step-off, syndesmotic instability, posterior talar subluxation, tibial plafond impaction. CT-based assessment of fragment morphology is increasingly used to guide management.18-21 Some studies suggest fixation of the posterior malleolus, regardless of size, to restore tibiotalar joint stability and improve contact pressure distribution.7 Conversely, other studies show posterior malleolar fixation in trimalleolar ankle fracture increases overall morbidity with increased tourniquet time, and wound healing complications, and did not eliminate the need for syndesmotic fixation.22 Literature supports a shift away from fragment size, and toward CT-guided, morphology and stability driven decision making for posterior malleolar fixation, recognizing potential benefits in tibiotalar stability while acknowledging increased operative morbidity and inconsistent avoidance of syndesmotic fixation (Figure 4).
5. Failure of Nonoperative Management
Patients initially managed nonoperatively require close surveillance with serial radiographs in the early post-injury period to ensure maintenance of fracture alignment and ankle mortise congruency. Any loss of alignment, interval displacement, or development of talar subluxation during follow-up warrants reconsideration of surgical fixation in a timely manner.
Conservative Management: When Not to Fix an Ankle Fracture
Nonoperative management is not “do nothing.” It is an active treatment plan with defined checkpoints. Early follow-up (often 5–10 days) to reassess edema/skin, alignment on repeat radiographs (and weight-bearing radiographs when appropriate), patient compliance and safety with weight-bearing plan. Conversion to surgical intervention is warranted when there is any loss of reduction, new mortise incongruity, progressive medial clear space widening with talar shift, and an inability to maintain alignment due to patient factors.
1. Stable Isolated Weber B Fractures
Multiple prospective studies support nonoperative management of isolated Weber B ankle fractures when weight-bearing radiographs demonstrate a stable ankle mortise and no evidence of medial or syndesmotic instability.4-6,8 In these cases, functional treatment with early protected weight-bearing results in clinical and radiographic outcomes comparable to operative fixation. Nonoperative management avoids the risks inherent to surgery, including wound complications, infection, hardware irritation, and the potential need for secondary procedures, while allowing for earlier mobilization and return to activity. Careful patient selection and close radiographic follow-up remain essential, as delayed displacement may occur in fractures with unrecognized instability or evolving ligamentous injury.
2. Select Elderly or Medically Frail/Compromised Patients
The Ankle Injury Management (AIM) trial demonstrated that in older adults with unstable ankle fractures, close contact casting produced functional outcomes equivalent to surgery at 6 months, with fewer wound complications and surgical morbidity.23 Subsequent literature emphasizes an individualized approach to management that accounts for medical comorbidities, skin integrity, bone quality, baseline mobility, cognitive status, and the patient’s ability to tolerate anesthesia and comply with postoperative restrictions.24 In appropriately selected patients, nonoperative management may provide acceptable outcomes while minimizing complications which disproportionately affect older and medically complex populations.
3. High-Risk Patients
Patients with severe peripheral vascular disease, diabetes with compromised soft tissue envelopes, immunosuppression, or poor wound-healing potential may benefit from nonoperative care even for fractures typically treated surgically, provided an anatomic reduction can be achieved and maintained. In these high-risk populations, the morbidity associated with surgical exposure, fixation, and potential wound complications may outweigh the benefits of operative intervention. A landmark long-term study demonstrated acceptable outcomes in displaced bi- and trimalleolar fractures treated nonoperatively when alignment was preserved.25 These findings highlight the importance of individualized decision-making prioritizing bone healing risk, soft tissue viability, and the capacity to maintain reduction.
Practical Treatment Algorithm
In general, our team follows the pathways below.
Surgical fixation is favorable when:
• Mortise incongruity exists or develops over time
• Functional instability is demonstrated
• Syndesmotic instability is present
• Posterior malleolus fracture compromises stability
• Open injury or fracture-dislocation
Nonoperative management is reasonable when:
• Mortise alignment is stable on weight-bearing imaging
• Patient-specific risks outweigh surgical benefits
• Anatomic reduction can be achieved and closely monitored
Conclusion
The decision to fix or not fix an ankle fracture is no longer dictated by fracture pattern alone. Instead, ankle stability, talar congruency, and patient-specific considerations guide modern management. Advances in functional imaging, evolving understanding of syndesmotic and posterior malleolar biomechanics, and high-quality randomized trials have expanded the role of nonoperative treatment in select patients. For foot and ankle physicians, applying an evidence-based, individualized approach optimizes outcomes while minimizing unnecessary surgical risk.
Dr. Bykowski is a Foot and Ankle Surgical Fellow at Illinois Bone and Joint Institute.
Dr. Burgess is the director of the Illinois Bone and Joint Institute Foot and Ankle Fellowship in Joliet, IL.
References
1. Ramsey PL, Hamilton W. Changes in tibiotalar area of contact caused by lateral talar shift. J Bone Joint Surg Am.1976;58(3):356-357.
2. Lloyd J, Elsayed S, Hariharan K, Tanaka H. Revisiting the concept of talar shift in ankle fractures. Foot Ankle Int. 2006;27(10):793-796. doi:10.1177/107110070602701006.
3. Michelson JD, Varner KE, Checcone M. Diagnosing deltoid injury in ankle fractures: the gravity stress view. Clin Orthop Relat Res. 2001;(387):178-182.
4. Weber M, Burmeister H, Flueckiger G, Krause F. The use of weightbearing radiographs to assess stability of supination-external rotation fractures of the ankle. Arch Orthop Trauma Surg. 2010;130(5):693-698.
5. Gougoulias N, Khanna A, Sakellariou A, Maffulli N. Supination-external rotation ankle fractures: stability a key issue. Clin Orthop Relat Res. 2010;468(1):243-251.
6. Gregersen MG, et al. Concomitant unstable and stable gravity stress tests on weight-bearing stable Weber B ankle fractures: a prospective noninferiority study. J Bone Joint Surg Am. 2023.
7. Lampridis V, Gougoulias N, Sakellariou A. Stability in ankle fractures: diagnosis and treatment. EFORT Open Rev. 2018;3(5):294-303.
8. Hoshino CM, Nomoto EK, Norheim EP, Harris TG. Correlation of weightbearing radiographs and stability of ankle fractures. Foot Ankle Int. 2012;33(2):92-98.
9. Zonneveld I, Hoogendoorn J. Variability in amount of weight-bearing while performing weight-bearing radiographs for assessing stability of ankle fractures. Eur J Trauma Emerg Surg. 2024 Aug;50(4):1521-1526. doi: 10.1007/s00068-024-02474-2. Epub 2024 Mar 2. PMID: 38430387; PMCID: PMC11458683.
10. Makwana NK, Bhowal B, Harper WM, Hui AW. Conservative versus operative treatment for displaced ankle fractures in patients over 55 years of age. J Bone Joint Surg Br. 2001;83(4):525-529.
11. Lauge-Hansen N. Fractures of the ankle. II. Combined experimental-surgical and experimental-roentgenologic investigations. Arch Surg. 1950;60(5):957-985.
12. Hallbauer J, Schenk P, Herrmann L, Ullrich BW, Biedermann U, Wildemann B, Hofmann GO, Kohler FC. Objective assessment of syndesmosis stability using the Hook Test. J Clin Med. 2023 Jul 10;12(14):4580. doi: 10.3390/jcm12144580. PMID: 37510697; PMCID: PMC10380604.
13. Corte-Real N, Caetano J. Ankle and syndesmosis instability: consensus and controversies. EFORT Open Rev. 2021 Jun 28;6(6):420-431. doi: 10.1302/2058-5241.6.210017. PMID: 34267932; PMCID: PMC8246108.
14. Pogliacomi F, De Filippo M, Schiavi P, et al. Acute syndesmotic injuries in ankle fractures. Acta Biomed. 2021;92(1):e2021022.
15. Xu B, Hu J, Zhang C, et al. Comparison of suture button and syndesmotic screw for ankle syndesmotic injuries: a meta-analysis of randomized controlled trials. J Orthop Surg Res. 2023;18: (article).
16. Shimozono Y, Hurley ET, Myerson CL, Murawski CD, Kennedy JG. Suture button versus syndesmotic screw for syndesmosis injuries: a meta-analysis. Am J Sports Med. 2018;46(9):2315-2323.
17. Sanders DW, Manoli A II. Syndesmotic injuries: evaluation and management. J Am Acad Orthop Surg. 2014;22(6):372-382.
18. Miksch RC, et al. Open reduction and internal fixation of the posterior malleolus fragment: systematic review. J Clin Med. 2023.
19. Datta S, et al. A comprehensive review of recent trends in posterior malleolus fracture management. Cureus/Review (open access). 2024.
20. Bartoníček J, Rammelt S, Tuček M, Naňka O. Posterior malleolar fractures of the ankle. Eur J Trauma Emerg Surg. 2015;41(6):587-600.
21. Verhage SM, Hoogendoorn JM, Krijnen P, Schipper IB. When and how to operate the posterior malleolus fragment in trimalleolar fractures. Arch Orthop Trauma Surg. 2018;138(9):1213-1222.
22. Aravindan S, Tucker NJ, Prusick PJ, Mauffrey C, Parry JA. Open fixation of the posterior malleolus increases the morbidity of trimalleolar ankle fracture fixation. Eur J Orthop Surg Traumatol. 2023;33(6):2525-2532. doi: 10.1007/s00590-022-03455-0. Epub 2022 Dec 29. PMID: 36581699.
23. Willett K, Keene DJ, Mistry D, et al; AIM Trial Collaborators. Close contact casting vs surgery for initial treatment of unstable ankle fracture in older adults: a randomized clinical trial. JAMA. 2016;316(14):1455-1463.
24. Raschke MJ, et al. Ankle fractures in the elderly: new concepts. EFORT Open Rev. 2023;8(5):332-341.
25. Wei SY, Okereke E, Winiarsky R, Lotke PA. Nonoperatively treated displaced bimalleolar and trimalleolar fractures: long-term follow-up. Foot Ankle Int. 1999;20(7):404-407.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.