“Wound to Amputation” — How Insurance Companies Are Dictating the Clinical Care of Chronic Limb-Threatening Ischemia
From Salvageable to Non-Salvageable Limb
From Salvageable to Non-Salvageable Limb
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Ivana Dilip Kumar, Research Associate1; Anshita Kumari, MBBS2; Kusum Lata, MD, FACC, FSCAI3
1Research Associate, Sutter Health, Tracy, California (Under Sutter Health Modesto, California); Quarry Lane School, Dublin, California; 2Kasturba Medical College, Manipal, India; Research Associate, Sutter Health Tracy, California (Under Sutter Health Modesto, California); 3Interventional Cardiology; Board of Trustees, SCAI; Sutter Health, Tracy, California (Under Sutter Health Modesto, California)
Disclosures: The authors report no conflicts of interest regarding the content herein.
This work was not supported by funding agencies in the public, commercial, or not-for-profit sectors.
The authors can be contacted at:
Ivana Dilip Kumar, ivana.dkumar@gmail.com
Anshita Kumari, MBBS, anshitakumari0@gmail.com
Kusum Lata, MD, FACC, FSCAI, lata.drkusum@gmail.com
Chronic limb-threatening ischemia (CLTI) is the most severe form of peripheral vascular disease, particularly involving the below-knee arteries. Management of CLTI hinges on a combination of guideline-directed medical therapy and timely revascularization to avoid limb loss.1 However, below-knee arterial disease is particularly challenging: lesions are often long, calcified, small in caliber, and require significant technical skill, time, and advanced tools to treat effectively.2
In CLTI patients with diffuse below-the-knee arterial disease, endovascular therapy is frequently the primary revascularization strategy, in absence of suitability of surgery (lack of vein conduit, high surgical risk, lack of target vessel due to diffuse arterial disease).3
However, access to timely intervention can be disrupted by insurance denials, which have been shown to increase the risk of both minor and major amputations. Unclear and non-clinically grounded insurance policies reduce the likelihood that patients will receive timely, limb-saving interventions.
This case highlights the real-world consequences of delayed revascularization due to insurance denial, demonstrating how a potentially salvageable limb can deteriorate into a non-salvageable condition.
Case Presentation
A 68-year-old male presented with critical limb ischemia involving the left toes. Over several weeks, the wound worsened, spreading to adjacent toes. Debridement was performed by a podiatrist, who advised bone resection and potential vascular intervention to support healing (Figures 1-2).

Despite appropriate wound care and antibiotic therapy, the wound continued to deteriorate. His history included well-controlled diabetes (HbA1c 5.1), hyperlipidemia managed with statins and PCSK9 inhibitors (evolocumab), and hypertension under control. He was a nonsmoker, non-drinker, and had a healthy body mass index. He had undergone a previous left below-knee revascularization (anterior tibial and peroneal arteries) five months earlier, which had led to near-complete wound healing, until his recent deterioration.
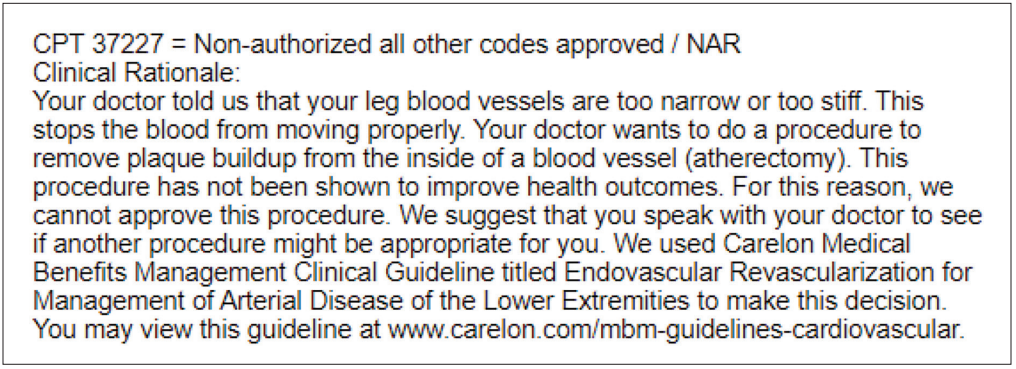
A request for urgent peripheral angiography to assess and treat worsening left lower extremity ischemia was denied by insurance. The reason cited was “revascularization in this condition has not been shown to improve outcomes” (Figure 3).
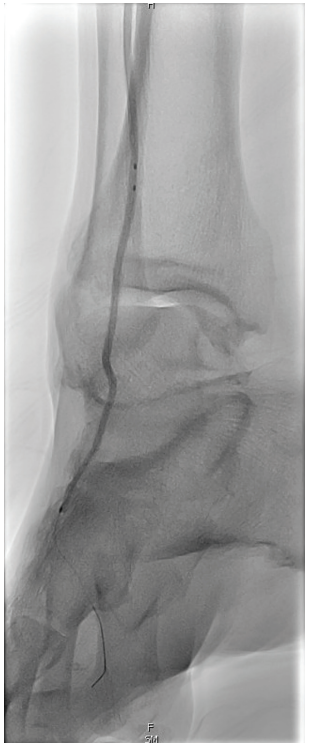
Over the following three months, repeated appeals and document submissions were made, with the patient’s clinical status worsening significantly (Figures 4-5).

Ultimately, after more than four months of delay, the insurance company approved the procedure (Figure 6).

Intervention
The revascularization was scheduled. Diagnostic angiography revealed:
- Moderate disease in the distal superficial femoral artery (SFA) and severe disease in the popliteal artery (Video 1).
- Critical, diffuse disease in the anterior tibial artery and total occlusions of the tibioperoneal trunk, peroneal, and posterior tibial arteries (Video 2).
angioplasty to improve microcirculation.
Intervention included:
- Laser atherectomy of the below-knee vessels.
- Pedal arch branch vessel angioplasty to improve microcirculation (Figure 7).
- Shockwave intravascular lithotripsy (IVL) with 4.0 mm and 5.0 mm balloons from the distal SFA to the anterior tibial and popliteal arteries.
- Prolonged percutaneous transluminal angioplasty (PTA) of the involved vessels, and drug-coated balloon angioplasty (DCB) in proximal anterior tibial and popliteal arteries (Videos 3-5).
Despite the complexity and prolonged delay, the patient tolerated the procedure well, and early signs of wound healing were observed within three weeks post intervention (Figures 8-9).

Discussion
The primary goal in managing CLTI is limb preservation, achieved through rapid wound healing and avoidance of infection or necrosis. Procedural success should not be measured solely by patency rates but by clinical outcomes, including avoidance of amputation, preservation of function, and survival.
Treating CLTI should be considered as urgent as treating ST-elevation myocardial infarction (STEMI). For CLTI, however, “door-to-balloon time” is measured in weeks, not months, so why the insurance barriers?
Key points:
- Revascularization in CLTI saves limbs and lives, and should not be delayed.
- Timely intervention is critical to achieving optimal outcomes.
- Procedure planning must remain in the hands of clinicians, not insurers or non-clinical administrators.
- The selection of tools (e.g., atherectomy, DCB, IVL) must be based on clinical need and operator expertise, not insurance limitations.
- Administrative burdens and repeated justifications consume valuable clinical time and risk burnout among vascular specialists.
- Insurance companies should be held accountable for delays that lead to preventable amputations.
- Physicians should be compensated for the non-clinical time spent fighting for necessary patient care.
Conclusion
CLTI affects over 6.5 million Americans, with below-knee arterial disease being the culprit in approximately two-thirds of cases. Without appropriate and timely revascularization, up to 25% of patients die within one year, and 50% within five years.4-6
Insurance approval for the procedure required nearly five months and multiple communications with the insurer.
While wound care and medical management are critical, revascularization, especially of both large and small vessels, is the cornerstone of limb salvage. Tools like atherectomy, prolonged PTA, DCB, and pedal arch angioplasty enhance luminal gain, improve microvascular flow, and promote durable healing.7,8
Insurance-driven delays jeopardize outcomes and burden the healthcare system. This case demonstrates that when care is dictated by non-clinical policies, salvageable limbs and lives are put at risk.
References
- Conte MS, Bradbury AW, Kolh P, et al; GVG Writing Group for the Joint Guidelines of the Society for Vascular Surgery (SVS), European Society for Vascular Surgery (ESVS), and World Federation of Vascular Societies (WFVS). Global vascular guidelines on the management of chronic limb-threatening ischemia. Eur J Vasc Endovasc Surg. 2019 Jul; 58(1S): S1-S109.e33. doi:10.1016/j.ejvs.2019.05.006
- Norgren L, Hiatt WR, Dormandy JA, et al; TASC II Working Group. Inter-society consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg. 2007 Jan; 45 Suppl S: S5-67. doi:10.1016/j.jvs.2006.12.037
- Farber A, Menard MT, Conte MS, et al; BEST-CLI Investigators. Surgery or endovascular therapy for chronic limb-threatening ischemia. N Engl J Med. 2022 Dec 22; 387(25): 2305-2316. doi:10.1056/NEJMoa2207899
- Pruthi S, Snyder DJ, Zilinyi RS, et al. Peripheral Matters | Bioresorbable Stents in Below-the-Knee Arterial Disease. Cardiology: A member publication of the American College of Cardiology. 2024 Nov 4: 28-29. Accessed February 27, 2026. https://bluetoad.com/publication/?i=834268&p=30&view=issueViewer
- Farber A, Rosenfield K, Menard MT. Clinical trials in chronic limb-threatening ischaemia. Br J Surg. 2023 Mar 30; 110(4): 397-398. doi:10.1093/bjs/znac465
- Fanaroff AC, Dayoub EJ, Yang L, et al. Development and description of a national cohort of patients with chronic limb-threatening ischemia. J Soc Cardiovasc Angiogr Interv. 2023 May 19; 2(4): 100982. doi:10.1016/j.jscai.2023.100982
- Tirziu D, Saleh A, Huang H, et al. Safety and efficacy of endovascular treatment modalities for below-the-knee arterial disease: a systematic review and network meta-analysis. J Endovasc Ther. 2025 Jun 30: 15266028251344809. doi:10.1177/15266028251344809
- Shahat M, Hassan A, Khalil MS, et al. Exploring the other side of the river: early and midterm outcomes of endovascular pedal arch revascularization in patients with chronic limb-threatening ischemia. J Endovasc Ther. 2024 Oct 28: 15266028241289034. doi:10.1177/15266028241289034