


Use of Discharge Summaries in Transitional Care: Addressing Hospital Documentation Gaps Through a Structured Checklist in a Skilled Nursing Facility
Abstract
Transitions of care from the hospital to skilled nursing facilities (SNF) represent high-risk periods for older adults, particularly when discharge documentation is incomplete. This clinical experience report describes the implementation of a structured discharge summary checklist at a 230-bed SNF. Data were collected over 8 weeks from 50 consecutive admissions. Use of the checklist revealed that 36% of patients had at least one medication discrepancy, 32% had pending results not highlighted in the discharge summary, and 32% had missing or unclear follow-up instructions. These findings underscore the limitations of hospital discharge summaries as a handoff tool and demonstrate how a structured checklist can systematically identify documentation gaps. By addressing deficiencies at admission, facility staff can improve patient safety, ensure continuity of care, and standardize communication. This low-cost intervention may be replicable across postacute care settings. The full checklist tool is included with this report to support implementation at other facilities.
Citation: Ann Longterm Care. 2026. Published online March 23, 2026.
DOI:10.25270/altc.2026.31.001
Transitions from the hospital to a skilled nursing facility (SNF) represent a vulnerable period for older adults with multiple comorbidities. Communication failures between hospital teams and postacute care providers contribute to medication errors, missed follow-up appointments, adverse outcomes, and rehospitalizations.1,2 Hospital discharge summaries are intended to serve as the cornerstone of hospital-to-facility communication, yet studies demonstrate that they are frequently delayed, incomplete, or lack essential information.3,4 Additionally, pending laboratory or imaging results may not be included, medication changes may not be clearly explained, and outpatient follow-up plans may be missing or inconsistent. As a result, skilled nursing facilities often receive patients with incomplete clinical handoffs, leaving admitting providers to resolve documentation gaps. This undermines continuity of care and places patients at risk for preventable complications. This report describes a clinical initiative to improve transitional care at an SNF through implementation of a structured discharge summary checklist used during admission review.
Setting and Participants
The project was conducted at a 230-bed long-term care and SNF in Washington, DC. The patient population comprised adults aged 65 to 85 years admitted for postacute rehabilitation following hospitalization. Over an 8-week period, 50 new admissions were reviewed using the checklist.
Intervention
The medical director and nursing leadership team developed a hospital discharge summary review checklist (Figure) to be completed within 24 hours of admission to guide staff in reviewing essential clinical components. The checklist addressed medication reconciliation, pending results, follow-up needs, special instructions, and advance care planning.
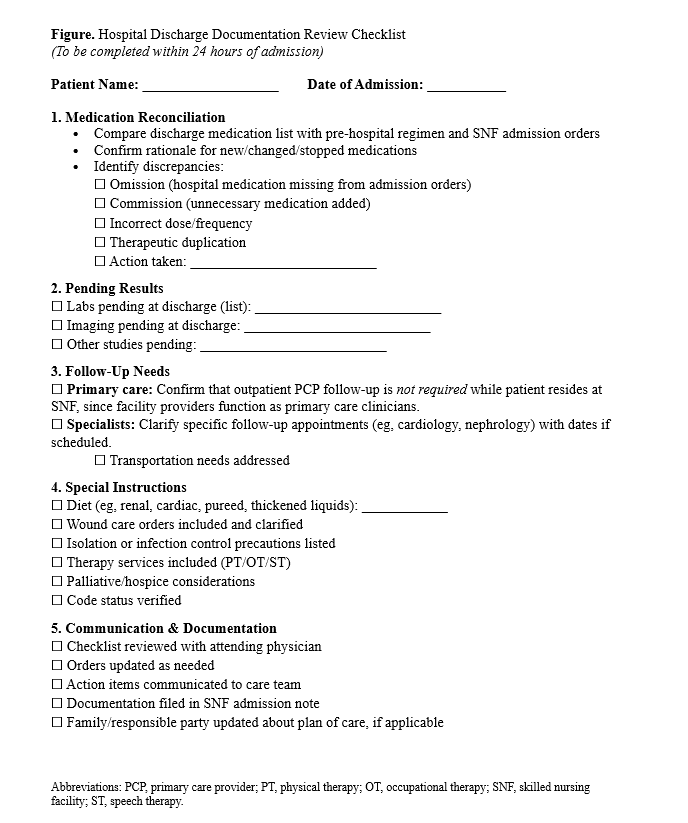
Notably, the follow-up section was adapted for the SNF setting, as patients were designated to follow up with facility providers; therefore, outpatient primary care visits were not required during the SNF stay. Instead, the checklist prioritized specialist referrals, therapy services, and post-SNF care planning.
Process
Upon each new admission, nursing staff ensured that the hospital discharge summary was included in the patient’s record. The admitting nurse and physician jointly applied the checklist during the admission evaluation. The checklist became part of the standard admission workflow and was consistently completed within 24 hours of admission. The average time required to complete the checklist was approximately 10 to 15 minutes once staff became familiar with the workflow. The checklist was used by multiple admitting providers, including attending physicians and advanced practice providers. Findings were documented in the medical record and communicated to the nursing supervisor and interdisciplinary care team. When discrepancies or missing information were identified, nursing staff directly contacted the discharging hospital for clarification. Beyond serving as a patient safety measure, the checklist also functioned as an educational tool for nursing staff and resident trainees during interdisciplinary rounds.
Evaluation
The intervention was piloted over an 8-week period involving 50 consecutive admissions. Data collected included the frequency of discrepancies, the proportion of issues attributable to incomplete hospital documentation, the frequency of admissions requiring follow-up clarification from hospital teams, and staff perceptions of checklist usability and clinical value.
The evaluation focused on identifying documentation gaps requiring follow-up rather than measuring downstream clinical outcomes. The project did not specifically track adverse drug events, missed abnormal results, or readmissions attributable to documentation gaps, though these represent important areas for future study. This initiative was conducted as part of the facility’s quality improvement efforts consistent with Quality Assurance and Performance Improvement (QAPI) principles.
Results
Among the 50 admissions reviewed, 36% of patients had at least one medication discrepancy, most often omissions or duplicate therapies, 32% of patients had pending results that were not highlighted in the discharge summaries, and 32% had missing or unclear follow-up plans. Another 32% had incomplete or inconsistent special instructions, including wound care protocols, diet orders, and therapy referrals. These findings required additional clarification from discharging hospitals or modification of admission orders to ensure safe continuation of care.
Staff Feedback
Feedback from interdisciplinary staff, including attending physicians, advanced practice providers, and nursing leadership, was collected through structured group discussions in quality meetings and interdisciplinary rounds. Staff consistently reported that the process improved the systematic review of discharge documentation, facilitated workflow integration, enhanced interdisciplinary communication, and increased confidence in managing new admissions. They also noted recurring deficiencies in hospital discharge documentation, reinforcing the ongoing need for standardized transition processes.
Discussion
The implementation of a structured checklist at the time of SNF admission provided a practical mechanism for identifying gaps in hospital discharge documentation. Medication discrepancies, unclear follow-up instructions, and unacknowledged pending results were common and posed risks to patient safety. By requiring systematic review of each domain and addressing issues proactively, the checklist functioned as a safety net, allowing providers to improve care continuity and reduce the likelihood of adverse events. Because it was integrated into existing workflows without the need for additional staff, the intervention presents a low-cost and feasible option for other SNFs.
Beyond its clinical utility, the checklist provided educational and cultural benefits. For nursing staff, it reinforced shared accountability for ensuring accurate information transfer. For physicians and trainees, it highlighted the limitations of current hospital handoff practices and emphasized the importance of proactive communication across care settings.
The findings also highlight the importance of bidirectional communication between SNFs and hospitals. Future efforts include sharing aggregated results with referring hospital partners and exploring collaborative quality improvement initiatives to strengthen discharge communication. Existing transitional care models, including tele-mentoring and collaborative transition programs, may provide useful frameworks for future implementation efforts.5
This project also aligns with national efforts to improve medication safety and transitional care for older adults and is conceptually consistent with broader age-friendly health system priorities focused on safe medication use and coordinated care transitions.
Limitations of the project include modest sample size, single-facility design, and lack of downstream outcomes, such as rehospitalization or medication adverse events. Future studies should evaluate clinical outcomes associated with documentation discrepancies and assess whether checklist implementation reduces avoidable readmissions.
Conclusion
Hospital discharge documentation is frequently incomplete, resulting in significant handoff deficiencies during transitions to SNFs. This clinical initiative demonstrates that implementing a structured discharge summary checklist in the SNF setting is both feasible and effective in strengthening transitional care. By systematically reviewing hospital discharge summaries at the time of admission, SNFs can identify and address deficiencies that might otherwise compromise patient safety, while also improving staff confidence in managing new admissions.
Broader adoption of structured review tools presents an opportunity to safeguard patients during these vulnerable transitions and promote a culture of accountability and quality improvement across the continuum of care. Incorporating such tools supports both patient safety and professional development, reinforcing best practices for interdisciplinary communication and standardized care processes.
Key Clinical Summary
- Transitions from hospital to skilled nursing facilities (SNFs) are often complicated by incomplete discharge documentation.
- In this quality improvement initiative, a structured discharge summary checklist identified frequent gaps, including medication discrepancies, unaddressed pending results, and unclear follow-up plans in over one-third of admissions.
- Implementing a standardized checklist at SNF admission improved identification of documentation deficiencies, supporting safer transitions of care and better continuity for older adults.
Affiliations, Disclosures & Correspondence
Author: Laila Alamgir, MD1,2
Affiliations:
1 Department of Internal Medicine, Howard University Hospital, Washington, DC
2 Unique Rehabilitation and Health Center, Washington, DC
Disclosure: The author reports no relevant financial relationships.
Address correspondence to:
Laila Alamgir, MD
Department of Internal Medicine
Howard University Hospital
2041 Georgia Avenue NW
Washington, DC 20060
Email: lalamgir@howard.edu
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Annals of Long-Term Care or HMP Global, their employees, and affiliates.
References
- Tjia J, Bonner A, Briesacher BA, McGee S, Terrill E, Miller K. Medication discrepancies upon hospital to skilled nursing facility transitions. J Gen Intern Med. 2009;24(5):630-635. doi:10.1007/s11606-009-0948-2
- Coleman EA, Parry C, Chalmers S, Min SJ. The care transitions intervention: results of a randomized controlled trial. Arch Intern Med. 2006;166(17):1822-1828. doi:10.1001/archinte.166.17.1822
- Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians. JAMA. 2007;297(8):831-841. doi:10.1001/jama.297.8.831
- Vasilevskis EE, Trumbo SP, Shah AS, et al. Medication discrepancies among older hospitalized adults discharged from post-acute care facilities to home. J Am Med Dir Assoc. 2024;25(7):105017. doi:10.1016/j.jamda.2024.105017
- Gleason LJ, Martinchek M, Long M, et al. An innovative model using telementoring to provide geriatrics education for nurses and social workers at skilled nursing facilities. Geriatr Nurs. 2019;40(5):517-521. doi:10.1016/j.gerinurse.2019.03.018

