


Assessment of Foam Support Surface Integrity in Long-Term Care Facilities
Abstract
Damaged support surfaces, such as mattresses, can increase the risk of infection and injury to residents in long-term care (LTC) facilities, yet there is limited information on the status of support surfaces and no standard of practice for routine assessment in these facilities. This analysis evaluated the condition of 31 746 support surfaces across 479 LTC facilities using visual examination and compression tests. Surfaces were examined for defined failure modes and categorized as needing immediate replacement (red), reassessment in 6 months (yellow), or suitable for continued use (green). The findings revealed that more than half (52.8%) of the surfaces required immediate replacement while 34.8% were identified as suitable for continued use. The most frequent failure modes were compression and holes or tears, often preceded by staining. The risk of surface failure can be calculated from surface age and rate of failure. About half of support surfaces are estimated to fail at 4 years of use, with a 73.5% increase in likelihood of failure each subsequent year. These results highlight the urgent need for standardized assessment of support surfaces to ensure resident safety, especially for older residents with increased risk of infection or injury.
Citation: Ann Longterm Care. 2026. Published online March 23, 2026.
DOI:10.25270/altc.2026.31.003
Residents in postacute long-term care (LTC) facilities, such as nursing homes, often have limited mobility, leading to a more sedentary lifestyle.1,2 As such, residents likely spend most of their time on support surfaces, such as mattresses and chairs.3 Support surfaces are categorized as high contact items in health care facilities that are subjected to heavy use.4,5 Frequent use and cleaning of support surfaces makes them particularly susceptible to wear and tear and accelerated damage, such as holes and tears. This damage not only affects visual appeal for residents, but can also have health consequences. Compromised support surfaces may lead to health care–associated infections (HAIs) and pressure injuries, both of which represent a significant risk to resident health as well as time and resources for health care facilities.6,7 Nursing home residents are particularly prone to infection and injury.8,9 Adequate information describing the condition of support surfaces in nursing homes over time is absent.
Damage to support surfaces can have a myriad of physical manifestations.5 Physical damage, which is caused by friction between the surface and resident, accounts for most support surface failure. In addition, heavy-duty cleaning products often cause chemical damage that further degrades support surfaces. Over time, friction or degradation may compromise the surface cover and expose the inner structure, making the surface vulnerable to pathogen adhesion and fluid ingress.10-12 Contamination of the inner structure eludes standard cleaning methods and makes the surface a potential source of HAIs.13,14 The significant risk of HAI from contaminated mattresses has been recognized by the US Food and Drug Administration (FDA) and the US Centers for Disease Control and Prevention (CDC).15,16 Both of these organizations have published literature on the risk of compromised support surfaces and recommend health care facilities address it with routine inspections and efficient repair or replacement.
Damaged support surfaces also pose the risk of pressure injuries to residents. Ideally, a support surface should minimize shear stress, control moisture and temperature, and distribute pressure.17-19 Damaged mattress covers create uneven surfaces that increase friction and moisture retention, which increases shear stress on the resident’s skin. Internal damage may affect the foam support to the extent that it cannot adequately distribute pressure and provide enough cushion. The European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel, and Pan Pacific Pressure Injury Alliance created a clinical guideline that recommends continuous observation of support surfaces for any damage that may affect function and increase risk of pressure injury development.19
Despite the known risk that compromised support surfaces pose to residents, there is limited precedent for health care facilities to perform routine assessments and systematically replace damaged support surfaces. To this end, we present a report on support surface assessments in LTC facilities in which we describe the modes and timelines of surface failure.
Methods
This study was exempt from Institutional Review Board oversight given that no human participants were involved.
Participating organizations were current and prospective customers of Medline Industries, LP, across the US who expressed interest in evaluating support surfaces in their facilities. An overview of the evaluations and supervision by onsite staff were described in written agreements. Two Medline representatives with nursing backgrounds performed the evaluations with designated facility champions. The onsite team was trained in performing standardized surface assessments, including a presentation on how to test and inspect each property of the surface. Mattress locations were recorded by room number and mattress identifier number (eg, 1/2 or a/b/c), or by specific location (eg, exam room or procedural unit). Only facility-owned mattresses owned were included in the inspections.
Residents who were able were asked to get up from the mattress so that linens could be removed for inspection. Support surfaces occupied by residents who could not get out of bed were not assessed. Visual inspection focused on sagging in the middle of the surface and defects along the edges of the frame. Stains, discoloration, tears, indentations, and thinning on any side of the mattress were noted. Photos documented these findings. Zippers were tested for function, and any information on the surface tag, including manufacturer, date of production, and size was recorded. If heavy staining or visible wear was observed, the inside of the mattress was inspected for contamination using a light source. Any damage to the surface cover or signs of contamination, discoloration, malodor, and moisture were noted.
Compression tests were also performed by pressing fists downward into the mattress using full body weight (Figure 1). The test was done in rows, starting at the head of the surface and continuing down to the foot of the surface. Each row was assessed 2 to 3 times across the width, separated by 8 to 10 inches in length. For each compression, the bounce-back and ability to feel the frame was noted. An overused surface with compromised integrity did not bounce back as fast as a firm surface. Surfaces were deemed compromised if the frame could be felt through the surface or if any fluid seeped out during the compression test.
Figure 1. Example of Compression Testing of a Support Surface

If any of these conditions were observed (ie, loss of compression, fluid leakage, sagging, indentation, tears, discoloration, thinning), the surface was assigned a red tag, indicating immediate replacement. If none of the conditions were observed, the surface was assigned a green tag, indicating suitable for use. If slight compression loss and staining were observed, specifically if the mattress bounced back but there was still sagging, the surface was assigned a yellow tag, indicating reassessment needed in 6 months). These assessments were recorded on paper or phone tracker application, and then compiled into a report that was presented in the facility.
Data Analysis
All analyses were conducted with 95% confidence in Stata 17.0 (StataCorp. 2021. Statistical Software Release 17. College Station, TX. StataCorp LLC). All variables were analyzed for normality to determine appropriate testing using measures of skew, kurtosis, and histogram examination. Most of the analyses presented are descriptive statistics (sample N and percentage). When inferential statistics were used, the statistical tests used were based on the distribution of the data for each variable and are detailed in the results section below for each separate test conducted.
Results
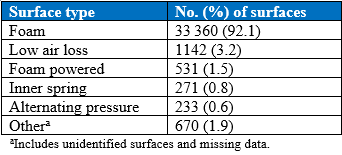
Assessments were conducted in nursing homes, assisted living centers, rehab hospitals, hospitals with LTC facilities, behavioral health facilities, home health agencies, physician offices, and several other facilities (Table 1). The categories of surface types assessed were foam, low air loss, foam powered, inner spring, alternating pressure, and gel, with a small number identified as “other” or “invalid” due to missing data (Table 2). Because most assessments were conducted on foam mattresses found in nursing homes, the analysis focused on this subset of data. The final dataset for this study included 31 746 foam mattresses from 479 nursing homes.
Table 1. Distribution of Facility Types Assessed (N=521)
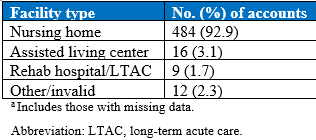
Table 2. Distribution of Support Surface Types Assessed (N=36,207)
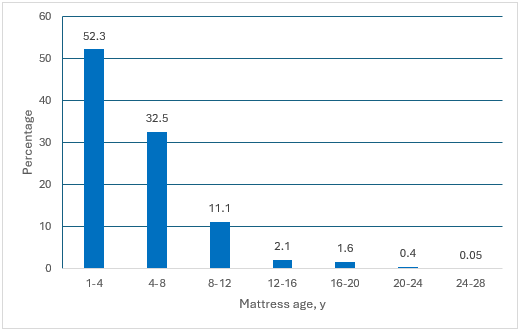
The average number of mattresses inspected per nursing home was 133.1 (SD, 75.2; range, 1–816). Most mattresses assessed were between 1 and 12 years old, with 52.3% aged 1 to 4 years; 32.5% aged 4 to 8 years, and 11.1% aged 8 to 12 years. The overall average age of mattresses was 7.1 years (SD, 3.7; range, 0–26 years) (Figure 2).
Figure 2. Distribution of Mattress Age
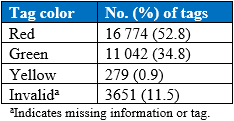
Of the total mattresses assessed, more than half (16 774, or 52.8%) were tagged red, indicating the need for immediate replacement due to one or more failures. In contrast, 279 (0.9%) were tagged yellow for reinspection in 6 months, and 11 042 (34.8%) were tagged green and approved for continued use. The remaining 3651 (11.5%) were categorized as invalid for missing information or tags (Table 3).
Table 3. Frequency of Tag Color of Foam Mattresses Assessed (N=31746)
The average mattress age for each of the tag designation was as follows: green-tagged surfaces averaged 3.3 years (median, 2; range, 0-29); yellow-tagged surfaces averaged 4.3 years (median, 3; range, 0-29); and red-tagged surfaces averaged 8.8 years (median, 6; range, 0-29). The average age of green-tagged surfaces is on average lower statistically lower than that of the red- and yellow-tagged surfaces (Figure 3). Figure 4 shows examples of the inspection failure modes.
Figure 3. Age Distribution of Assessed Foam Mattresses by Inspection Tag Color
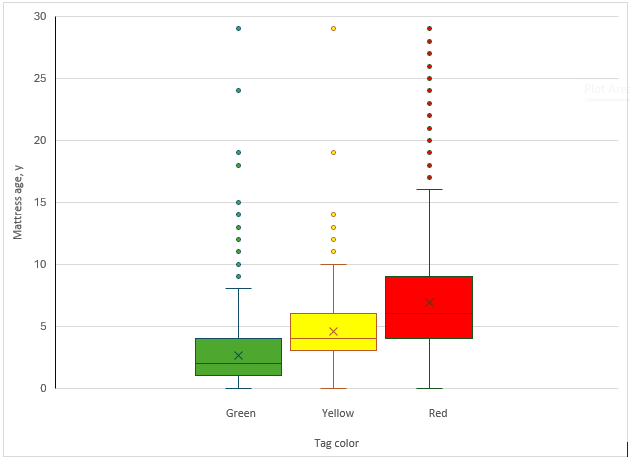
The horizontal line inside each box indicates the median, and the “X” inside the boxes indicates the mean. The lower and upper ends of the boxes represent the first and third quartiles. Whiskers extend to the smallest and largest values within the defined range, and data more extreme than the whiskers are plotted individually as outliers (dots). Green-tagged mattresses were generally younger (median, 2 years) than yellow-tagged (median, 3 years) and red-tagged mattresses (median, 6 years).
Figure 4. Examples of Inspection Failure Modes of Assessed Surfaces
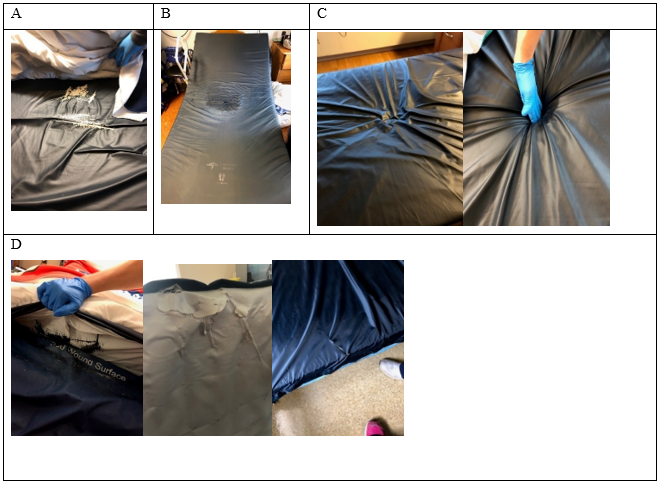
A, Thinning, fraying cover, which can damage the skin. B, Soiling, which may lead to internal contamination and expose patients to potentially harmful pathogens. C, Compression. D, Holes, tears, and rips, which may accelerate surface deterioration, compromise internal components, and allow fluid and contaminants ingress. All pictures were taken from March to June, 2019.
The amount and type of failure modes observed were quantified and compared. Of the red-tagged surfaces, 7634 (24.1%) had a single failure mode, 5319 (16.7%) had two failure modes, and 3821 (12%) had three or more failure modes (Table 4). Among these, the most common single failure modes were compression in 5015 (65.7%) surfaces, holes/tears/fraying in 1788 (23.4%) surfaces, and staining in 424 (5.6%) surfaces (Table 5). Among the yellow-tagged surfaces, the most frequent failure mode by far was staining in 257 (93.5%) surfaces, which suggests that staining may precede the failure modes observed in red-tagged surfaces (Table 6). Figure 5 shows the correlation matrix of red-tagged mattresses with double failure modes.
Table 4. Frequency of Failure Category for Red-Tagged Surfaces
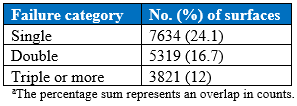
Table 5. Frequency of Single Failure Mode by Red Tag
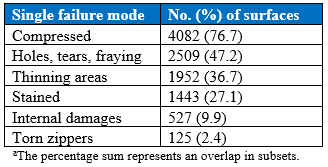
Table 6. Frequency of Single Failure Mode by Yellow Tag
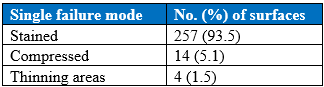
Table 7. Frequency of Failure Modes in Surfaces With Multiple Failures
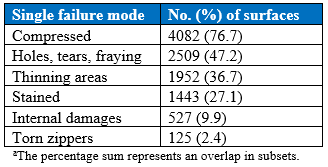
Figure 5. Correlation of Red Tags With Double Failure Modes for Assessed Surfaces
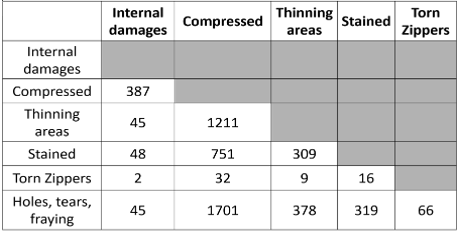
Each cell shows the number of mattresses that exhibited both failure modes listed in the corresponding row and column. Rows and columns represent failure types: internal damages, compression, thinning areas, staining, torn zippers, and holes/tears/fraying. Higher counts indicate more frequent co-occurrence of failure modes. Shaded cells indicate diagonal or noncomparable combinations.
The most common pair of failure modes was compression and holes/frays/tears (65.69% and 23.42%, respectively). This is consistent with the most frequently observed single failure modes. Compression was also found to be highly correlated with thinning, torn zippers, and internal damage (Figure 4).
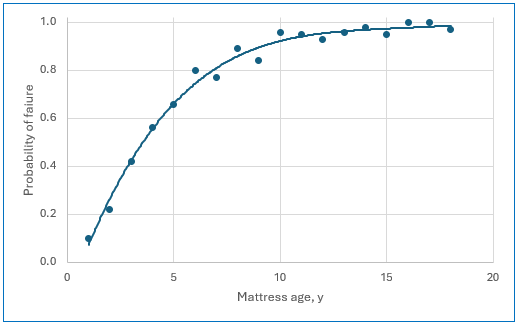
The support surface analyses were also used to correlate age and failure rate, which allowed for calculation of failure risk with each year of use in the postacute setting. From this, a “half-life” at which risk of failure is 50% was determined to be approximately 4 years (Table 8, Figure 6). For each year of use, risk of failure increased by 73.5%. These data highlight the necessity of routine support surface inspection to identify failed surfaces and replace them more efficiently.
Table 8. Half-Life of Foam Mattresses in Nursing Homes
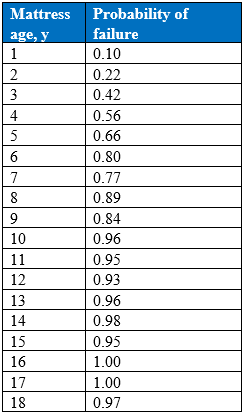
Figure 6. Half-Life of Foam Mattresses Assessed
Discussion
Monitoring the condition of support surfaces in health care facilities has increasingly gained attention as a critical factor to providing quality resident care. Many residents, particularly those with limited mobility, may spend years confined to their mattresses during their stay, prolonged use on damaged surfaces may increase the risks of infection and pressure injuries.3 These risks increase with resident age, making mattress integrity especially relevant for older adults in nursing homes.8,9 However, most postacute health care facilities lack protocols for routine assessment and replacement of support surfaces. The motivation behind this study was to report on surface integrity, age, and common failure modes in a postacute health care setting, with the goal of better defining when and how support surfaces fail and thus highlight the need for more frequent surface assessments.
This study found that more than 50% of support surfaces in the participating postacute health care facilities were not suitable for continued use. Of these surfaces, about 30% had more than one failure mode, with compression and holes or tears as the most common. A small percentage of the surfaces were marked for follow-up assessment, most of which presented with staining. Notably, staining often appeared before other failure modes (eg, compression and holes/tears), suggesting it be any early indicator of surface failure. Foam support surfaces had a “half-life” of 4 years, with a 73.5% increased risk of failure with each subsequent year of use.
To our knowledge, no study has established a direct correlation between damaged support surfaces and risk of hospital-acquired conditions (HACs). However, compromised support surfaces are shown to increase infection and may contribute to pressure injury development.10-12, 17-19 Compromised mattresses are subject to contamination via fluid leakage that standard cleaning techniques cannot adequately disinfect.13,14 Furthermore, damage to the mattress cover may also affect the surface microenvironment, increasing friction and shear stress on the resident’s skin. Any internal damage or degradation can also impair the distribution of pressure, further elevating the risk of a pressure injury.
Reducing HACs is a top priority for health care facilities due to the significant health risk and burden they pose to both health care providers and residents. In postacute health care facilities that treat residents with high risk for HACs, is it critical to monitor potential sources of HACs, such as damaged mattresses. HACs occur more frequently among older adults, often due to limited mobility, multiple comorbidities, and immunosenescence.8,9 The prevalence of HAIs has increased from 7.4% to 11.5% among residents aged 85 years and older.20 HAIs affect approximately 1 to 2.6 million US nursing home residents, with one in every 43 residents contracting at least one infection per day.22 Many of the most common microorganisms responsible for HAIs in older residents are multidrug-resistant, making infection a leading cause of death in nursing homes.23 On average, HAIs cost $31 000 to treat and account for $28.4 billion in direct medical costs in the US.24 Pressure injuries affect approximately 11% of US LTC residents, with higher risks seen among residents with comorbidities or chronic conditions.25-27 These injuries cost between $20 900 and $151 700 to treat per resident, adding up to approximately $3.3 billion per year for US nursing homes. In contrast, a ballpark cost estimate of for a standard foam support surface is $250. The cost of treating one resident with a pressure injury or HAI is equivalent to purchasing 83 to 124 new mattresses, respectively. This suggests that replacing damaged mattresses is a cost-effective method for reducing HACs and saving health care facilities’ time and resources.
The results of this study closely align with a similar analysis we performed in an acute care (hospital) environment. Using 2019 data, that assessment evaluated the integrity of 5121 surfaces across 85 health care facilities and found that 59% were red-tagged as unsuitable, and less than 33% were considered suitable for use (green tags). As in this postacute care study, the most common failure modes were holes, tears, and thinning, with staining appearing as a leading indicator of mattress failure. Interestingly, the estimated half-life of foam support surfaces in acute care was also 4 years.28
This study has several limitations. First, these surface assessments were qualitative in nature and conducted by multiple personnel, which may have caused inconsistencies. To help reduce the risk of inconsistencies and preserve data integrity, the process was standardized by the development of data collection tools. To help mitigate subjectivity, the process used in our study design has significant parallels to the methods and definitions set forth by the National Pressure Injury Advisory Panel Support Surface Standards Initiative (S3I). The assessment process uses the hand check method to evaluate mattress bottoming out. Second, the methodology may be subject to inherent bias. These study methods, which include hand checks, have been historically used and remain the only readily available method for clinicians and caregivers.
There may be erroneous perceptions of the durability of foam support surfaces. Although mattresses carry manufacturer warranties of up to 10 years,29 these typically only cover manufacturing defects—not the wear and tear of extended daily use. The American Hospital Association recommends replacing surfaces every 5 years,30 but our data suggest that 4 years is more accurate. We hope nursing home administrators interpret these findings as a call to proactively inspect support surfaces. Ideally, personnel who are responsible for bedding changes could be trained to identify signs of aging, such as wear, reduced height/thickness, discoloration, altered cover integrity, altered seams and zipper/zipper cover flaps, and odor, as described in the Methods section of this report. Notably, staining was by far the most frequent failure mode associated with yellow tag designations, suggesting that staining could be a leading indicator of failure for foam support surfaces. Given that staining is relatively easy to identify during routine bedding changes, staff should identify stained mattresses for continued monitoring and timely replacement as soon as they are compromised. Routine inspection of support surface damage has the potential to minimize infection risk and support efforts to maintain residents’ skin integrity.
Conclusion
The FDA and CDC, among other organizations, have recognized the risks that damaged support surfaces pose to residents and issued guidelines for mattress replacement.15,16,26 This study presents a standardized method for support surface assessment, identifies common failure modes, and calculates a “half-life” to predict the risk of mattress failure with each year of use. These findings can help postacute health care facilities better understand how and when mattresses fail so that they can be monitored and replaced more efficiently. Proactively removing compromised surfaces can reduce the amount of time residents spend on compromised support surfaces, potentially reducing the risk of pressure injuries and infection.
Key Clinical Summary
- More than half of support surfaces in long-term care facilities (52.8%) were found to be unsuitable for use, with common failure modes including compression and tears, often preceded by staining.
- Mattress failure risk increased substantially with age, with an estimated “half-life” of 4 years and a 73.5% higher likelihood of failure for each additional year of use.
- These findings underscore the need for standardized, routine assessment and timely replacement of support surfaces to reduce infection risk and pressure injuries in vulnerable LTC populations.
Affiliations, Disclosures & Correspondence
Gregory Manista, MD, MS1 • Tochukwu Ikpeze, MD1 • Lisa Nicholson, PhD1 • Joyce Black PhD, RN, FAAN2 • Thomas Koshy, PhD3
Affiliations:
1 Department of Medical Affairs, Medline Industries, LP, Northfield, IL
2 Florence Neidfelt Professor in the College of Nursing at the University of Nebraska Medical Center in Omaha, Nebraska
3 Beeatus Solutions, Inc., Palatine, Illinois
Disclosure:
The authors report no relevant financial relationships. Except for Dr Black, all authors were employees of Medline Industries, LP, at the time of this research and/or manuscript preparation. Dr Black received no financial compensation for her contribution to this manuscript.
Address correspondence to:
Gregory Manista, MD, MS
Email: gregorymanistamd@gmail.com
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Annals of Long-Term Care or HMP Global, their employees, and affiliates.
References
- Resnick B, Galik E, Boltz M, et al. Physical activity and function in assisted living residents. West J Nurs Res. 2018;40(12):1734-1748. doi:10.1177/0193945918764448
- Fazio S, Stocking J, Kuhn B, et al. How much do hospitalized adults move? A systematic review and meta-analysis. Appl Nurs Res. 2020;51:151189. doi:10.1016/j.apnr.2019.151189
- Buttigieg SC, Abela L, Pace A. Variables affecting hospital length of stay: a scoping review. J Health Organ Manag. 2018;32(3):463-493. doi:10.1108/JHOM-10-2017-0275
- Marks B. Uncovering the prevalence of damaged mattresses. Published February 29, 2016. Accessed November 8, 2025. https://www.ahe.org/uncovering-prevalence-damaged-mattresses
- Marks B, de Haas E, Abbound T, et al. Uncovering the rates of damaged resident bed and stretcher mattresses in Canadian acute care hospitals. Canadian J Infect Control. 2018;33(3):171-175.
- Hooker EA. Hospital mattress failures: a hidden patient danger. Infect Control Hosp Epidemiol. 2023;44(3):501-503. doi:10.1017/ice.2021.486
- Li X, Lam I, Teska P, Grinstead D, Becker L. Infection risks associated with damaged mattresses and management strategy using repair patches. Infection Control Tips. Published May 4, 2021. Accessed November 8, 2025. https://infectioncontrol.tips/2021/05/04/infection-risks-associated-with-damaged-mattresses-and-management-strategy-using-repair-patches/
- Cristina ML, Spagnolo AM, Giribone L, Demartini A, Sartini M. Epidemiology and prevention of healthcare-associated infections in geriatric residents: a narrative review. Int J Environ Res Public Health. 2021;18(10):5333. doi:10.3390/ijerph18105333
- Chung ML, Widdel M, Kirchhoff J, et al. Risk factors for pressure injuries in adult residents: a narrative synthesis. Int J Environ Res Public Health. 2022;19(2):761. doi:10.3390/ijerph19020761
- González, JF, Hahn MM, Gunn JS. Chronic biofilm-based infections: skewing of the immune response. Pathog Dis. 2018;76(3):41-48. doi:10.1093/femspd/fty023
- Ndawula EM, Brown L. Mattresses as reservoirs of epidemic methicillin-resistant Staphylococcus aureus. Lancet. 1991;337(8739):488. doi:10.1016/0140-6736(91)93420-e
- Fujita K, Lilly HA, Kidson A, Ayliffe GA. Gentamicin-resistant Pseudomonas aeruginosa infection from mattresses in a burns unit. Br Med J (Clin Res Ed). 1981;283(6285):219-220. doi:10.1136/bmj.283.6285.219
- Sexton T, Clarke P, O’Neill E, Dillane T, Humphreys H. Environmental reservoirs of methicillin-resistant Staphylococcus aureus in isolation rooms: correlation with resident isolates and implications for hospital hygiene. J Hosp Infect. 2006;62(2):187-194. doi:10.1016/j.jhin.2005.07.017
- de Andrade D, Angerami EL, Padavani CR. A bacteriological study of hospital beds before and after disinfection with phenolic disinfectant. Rev Panam Salud Publica. 2000;7(3):179-184. doi:10.1590/s1020-49892000000300007
- Covers for hospital bed mattresses: learn how to keep them safe. US Food & Drug Administration. 2017. Accessed November 8, 2025. https://www.fda.gov/medical-devices/hospital-beds/covers-hospital-bed-mattresses-learn-how-keep-them-safe
- Sehulster LM, Chinn RYW, Arduino MJ, et al. Guidelines for environmental infection control in health-care facilities. Recommendations from CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC). American Society for Healthcare Engineering/American Hospital Association; 2004. Accessed November 8, 2025. https://www.cdc.gov/infection-control/media/pdfs/Guideline-Environmental-H.pdf
- McNichol L, Mackey D, Watts C, Zuecca N. Choosing a support surface for pressure injury prevention and treatment. Nursing. 2020:50(2):41-44. doi:10.1097/01.NURSE.0000651620.87023.d5
- Terms and definitions related to support surface. National Pressure Injury Advisory Panel Support Surface Standards Initiative. Accessed September 15, 2023. https://cdn.ymaws.com/npiap.com/resource/resmgr/s3i/finalized_t&d_2025__2_.pdf
- Kottner J, Cuddigan J, Carville K, Balzer K, Berlowitz D, Law S, Litchford M, Mitchell P, Moore Z, Pittman J, Sigaudo-Roussel D, Yee CY, Haesler E. Prevention and treatment of pressure ulcers/injuries: The protocol for the second update of the international Clinical Practice Guideline 2019. J Tissue Viability. 2019 May;28(2):51-58.
- Oliveira AC, Viana RE, Damasceno QS. Contamination of hospital mattresses by microorganisms of epidemiological relevance: an integrative review. J Nurs UFPE Online. 2013;7(1):236-245. doi:10.5205/reuol.3049-24704-1-LE.0701201332
- “Healthcare-Associated Infections in the Elderly: What’s New” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5648009/#:~:text=The%20risk%20of%20developing%20a,age%20of%2065)(p%3D. Accessed on October 29, 2023.
- Current HAI progress report. US Centers for Disease Control and Prevention. Accessed October 30, 2023. https://www.cdc.gov/healthcare-associated-infections/php/data/progress-report.html
- Dorritie R, Quigley DD, Agarwal M, Tark A, Dick A, Stone PW. Support of nursing homes in infection management varies by US State Departments of Health. J Hosp Infect. 2020;105(2):258-264. doi:10.1016/j.jhin.2020.02.007
- Health topics. POLARIS. US Centers for Disease Control and Prevention. Published June 21, 2021. Accessed September 5, 2023. https://www.cdc.gov/policy/polaris/healthtopics/hai/index.html#:~:text=HAIs%20in%20U.S.%20hospitals%20have
- Stone A. Preventing pressure injuries in nursing home residents using a low-profile alternating pressure overlay: a point-of-care trial. Adv Skin Wound Care. 2020;33(10):533-539. doi:10.1097/01.ASW.0000695756.80461.64
- 2019 Top 10 Health Technology Hazards, Executive Brief. A Report from Health Devices. ECRI Institute; 2018. Accessed November 8, 2025. https://www.ecri.org/Resources/Whitepapers_and_reports/Haz_19.pdf
- Beeckman D, Serraes B, Anrys C, Van Tiggelen H, Van Hecke A, Verhaeghe S. A multicentre prospective randomised controlled clinical trial comparing the effectiveness and cost of a static air mattress and alternating air pressure mattress to prevent pressure ulcers in nursing home residents. Int J Nurs Stud. 2019;97:105-113. doi:10.1016/j.ijnurstu.2019.05.015
- Todd J, Manista G, Nicholson L, Ikpeze T, Black J, Koshy T. Assessment of support surface integrity in the acute healthcare setting. J Wound Ostomy Continence Nurs. 2025;52(3):181-189. doi:10.1097/WON.0000000000001182
- Noyed D. Mattress warranties. Sleep Foundation. Updated July 15, 2025. Accessed September 21, 2022. https://www.sleepfoundation.org/mattress-information/mattress-warranties
- Martonicz TW. Hospital mattress failure is a potential threat to patient safety. Infect Control Today. 2022;26(3). Accessed November 8, 2025. https://www.infectioncontroltoday.com/view/hospital-mattress-failure-potential-threat-patient-safety

