


Enhancing Sexual Well-Being in Long-Term Care: A Framework for Effective Guidelines
Abstract
Sexuality and aging are deeply connected yet often overlooked in long-term care facilities due to stigma and misconceptions. Recognizing this gap, an American long-term care nonprofit health organization formed a Sexual Health Committee to create guidelines supporting sexual expression for older adults, including those with cognitive impairment. The guidelines promote staff training, resident agency, and strategies for assessing consent and harm, using a two-tier model focused on personalized evaluation. A decision tree was created to help staff navigate complex situations in alignment with the guidelines. This article also shares common pitfalls to prepare staff for real-world challenges. Designed with flexibility in mind, the guidelines aim to support other facilities in starting conversations about sexual health and building their own guidelines or policies, aligning with person-centered care and the mission of honoring dignity in aging.
Citation: Ann Longterm Care. 2026. Published online March 23, 2026.
DOI:10.25270/altc.2026.31.002
Sexuality and aging are not mutually exclusive. Quite the contrary, intimacy and sexual expression are fundamental aspects of the human experience across a person’s lifespan.1 Yet, when a person enters a long-term care facility, sexuality and intimacy are often ignored, owing to assumptions that aging lessens a person’s desire and ability for sexual expression.2 In addition, staff and families may view residents’ sexual expression negatively and act in a prohibitive manner.3
Sexuality remains a contentious subject in most long-term care organizations and is therefore rarely discussed.4 However, it is important to provide access to information about sexuality for residents as well as caregivers. This is particularly crucial since access to information and services not only improves residents’ sexual health but also their overall quality of life.5 Research has shown that sexual engagement can confer many benefits among older adults, including physical (eg, pleasure, exercise, release of oxytocin or “cuddle hormone”); emotional (eg, improved mood, greater life satisfaction); cognitive (eg, improved cognitive test scores); relational (eg, reduced loneliness, improved feelings of intimacy); and spiritual (eg, feelings of gratitude).6 Despite these documented benefits, it remains exceedingly uncommon for long-term care facilities and healthcare organizations for older adults in the United States to have a formal sexual health policy, a set of guidelines, or even staff education about sexual health and aging.7 This gap in policy often leaves staff feeling unequipped to navigate issues of sexual health and wellness and further perpetuates stigma.8
At the healthcare division of a medical school–affiliated older adult healthcare and housing organization in the United States, a formal sexual health policies, staff education, and supportive guidelines were also absent. To address these gaps, a dedicated group of multidisciplinary team members formed a Sexual Health Committee (SHC), with a mission of encouraging healthy sexual expression for all older adults, including those with cognitive impairment. This article focuses primarily on the process of creating standardized guidelines for supporting sexual health and intimacy in long-term care communities, with the broader goal of encouraging other organizations to establish their own unique SHCs. Central to this process is understanding the cultural values of each organization, abiding by relevant local laws, and respecting the ethical codes of various professionals; it is the hope that other SHCs will individualize guidelines to their specific setting. We will review the goals of the guidelines, the frameworks used in their creation, and the strategies that long-term care team members can use to assess consent and potential harm when residents with cognitive or physical disabilities engage in sexual behavior. We will also share the challenges that we encountered, as well as future directions for the SHC. Of note, in a time of increased uncertainty around ageism-related research and clinical interventions, as well as other aspects of diversity, equity, and inclusion, it feels particularly important to advocate for the rights of those who may have less agency to make choices about their own bodies, identities, and sources of happiness.
Forming a Committee
Motivated to provide guidance to long-term care staff, as well as promote healthy engagement with sexuality for the facility’s residents, long-term care psychologist Rachael Arielly began recruiting a team of like-minded professionals to form the SHC. The team initially included staff from a range of disciplines, including nursing, chaplaincy, social work, and professional development. Two employees who were not affiliated with the organization also joined the team as volunteers (Nathalie Huitema and Sarah Rogers). The team conducted a needs assessment with nursing leadership to identify common issues related to patient sexuality. Notable issues were as follows:
- Staff encounters with sexual behaviors they considered aggressive
- Dealing with individuals masturbating in public areas
- The challenges of assessing consent
- Staff uncertainty about how to address sexuality, sexual expression, and sexual relationships
- A desire for practical guidelines and training for staff, families, and clinical coordinators
- A recommendation for a consultation team to review complex cases
Creating the Guidelines
The SHC felt it was important to create a set of guidelines that would both adhere to existing policies and reflect the mission and cultural values of the organization. As a nonprofit organization with Jewish roots, the long-term care organization prides itself on honoring older adults as promoted by the Fifth Commandment, and on its dedication to tikkun olam—the duty of healing the world.9 The SHC also wanted the guidelines to acknowledge and bring awareness to some of the intangible aspects of long-term care culture (eg, most common religious beliefs held by frontline staff, communication challenges). By anticipating points for potential pushback, the SHC could offer advice in navigating problems before they arise.
The guidelines were designed to encourage ongoing discussion, education, and support to ensure sustainable implementation. A key goal was for all direct care staff to feel a degree of expertise, or at least confidence, in managing issues of sexual health and expression. When the guidelines are paired with educational modules, the hope was to empower staff to respond appropriately, even when a member of the SHC was not present.
Core Principles
To ensure the guidelines were value-aligned, practical, and user-friendly, the SHC articulated a set of core principles as their foundation. Rooted in the issues identified by the nursing team’s needs assessment, these principles translate into actionable guidance for frontline staff and ensure that responses to sexual expression are consistent and informed. Written with the staff in mind, the guidelines provide contextual explanations of common questions and definitions where needed, alongside practical steps that align with the organization’s values and sexuality frameworks.
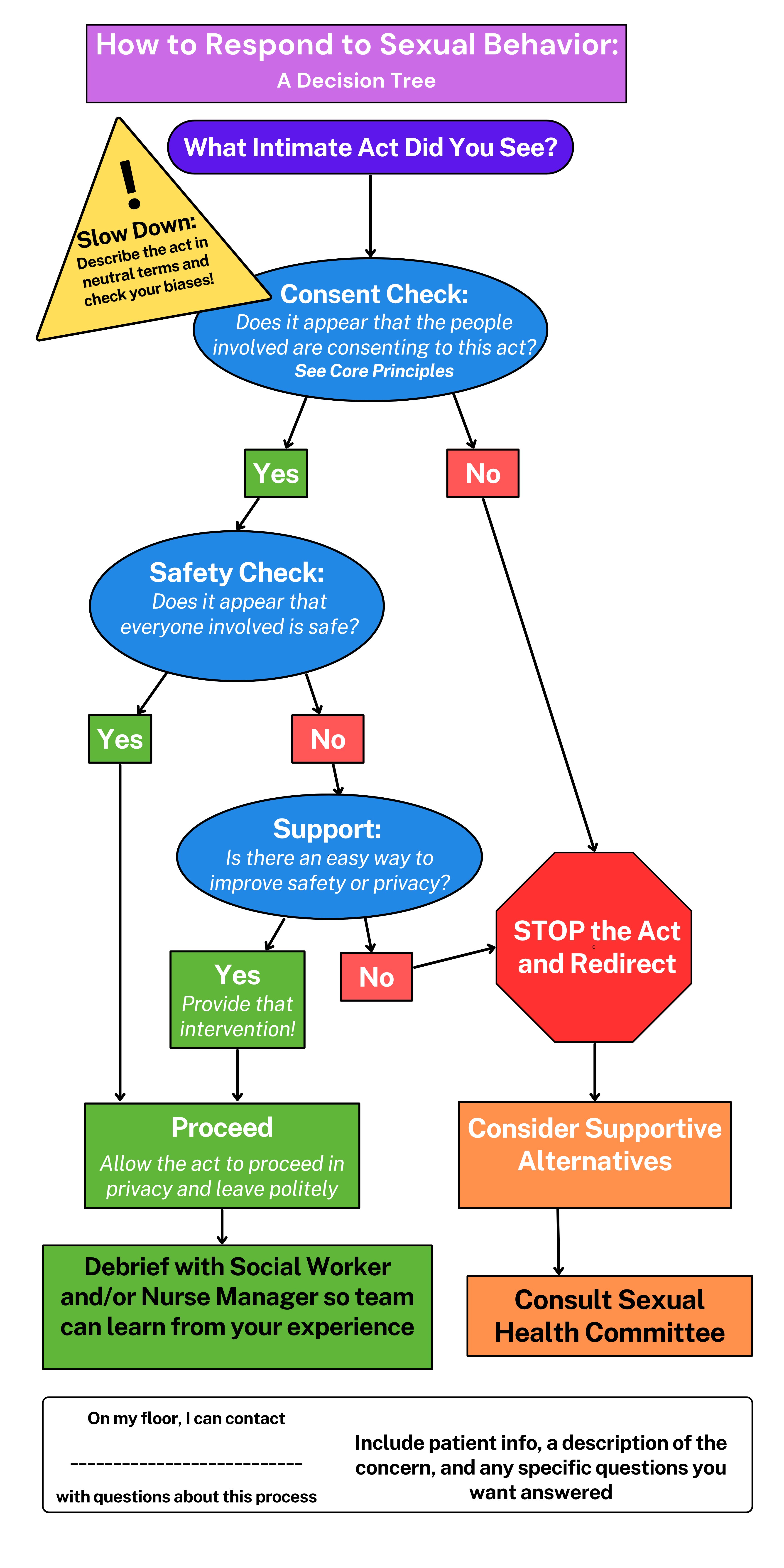
To support staff implementation, a decision tree (Figure) was developed based on these core principles. The decision tree helps guide staff through real-life situations with an easily accessible framework for navigating sexual expression situations. This tool helps staff engage in autonomous decision making by asking questions informed by the core principles. Below, we discuss some of these core principles identified in the guidelines.
How do we prepare staff to engage in older adults’ sexual expression?
This question shifts the guidelines from words on a page to integration with the community fabric. It starts with presenting them in an accessible and consistent manner throughout the organization, with the goal of empowering staff and older adults (and their families) to engage in informed decision making surrounding sexual expression. This requires administrative support, such as setting aside time and resources to provide staff with continuing education as well as create opportunities for older adults to cultivate social connections.
Staff training can take on multiple forms, such as interactive PowerPoint presentations, one-to-one check-ins with educators, and in-depth case reviews with the SHC. All training starts with sharing the guidelines and supplemental tools (eg, decision tree) with staff. This foundational knowledge is critical to support staff as they navigate complex situations surrounding older adults’ sexual expression. Training includes teaching staff how to provide care that respects the expressed wishes of the older adult, while remaining grounded in their own beliefs. Staff also learn about the connections between sexual expression and improved health and positivity, which can increase their investment in this paradigm shift.
Case reviews with the SHC are a pivotal learning opportunity for staff to ask complex questions, dissect nuanced situations, and receive support to improve older adults’ quality of life.
How do staff promote agency in older adults’ sexual expression?
With training and administrative support, staff have the unique opportunity to support older adults’ sexual engagement, while mindfully adhering to ethical and legal guidelines. This includes making older adults aware of their rights and the resources they can access to safely express their sexuality. The guidelines incorporate principles of respecting the staff (eg, clarity on staff boundaries/standards of practice) and respecting older adults (eg, privacy measures of knocking on doors before entering, discretion when charting sexual concerns). Concrete support from staff can include providing older adults with sexually explicit technologies and materials, private spaces upon request, and preparation for and cleanup after sexual activities.
How do staff determine sexual consent in people with cognitive impairment?
To illustrate the practical application of a consent framework in aged care policy, we highlight a central principle that informs our approach: that determining sexual consent in older adults with cognitive impairment is a nuanced process requiring both sensitivity and structure. To counter this, we introduce the concept of sexual consent potential,4 which reframes consent as a dynamic process. This concept aligns with person-centered care values and supports older adults in exercising agency within the bounds of safety and ethical responsibility. In practice, this approach is operationalized through a two-tiered consent determination process.
Tier 1 provides frontline staff with a set of guiding criteria to assess the capacity of individuals with no or mild cognitive impairment. The criteria emphasize core components of consent, including voluntariness, awareness, and the ability to communicate assent or dissent. To be considered capable of giving sexual consent, the older adult must have an affirmative response to all of the following criteria:
- Have basic knowledge of the nature of sexual activity
- Understand that sexual activity is voluntary
- Ability to resist coercion
- Ability to choose a socially acceptable time and place for intimate behavior
- Ability to initiate and stop intimate activity either independently or in response to the partner's expressed resistance
- Ability to respond to verbal, nonverbal, and/or behavioral communication from the sexual partner and express assent or dissent
A negative answer to one or more criteria does not necessarily prohibit sexual activity, but should serve as a benchmark for potential team intervention, the gathering of more information, or progression to Tier 2.
Tier 2 involves an interdisciplinary evaluation for individuals with more pronounced cognitive impairment. This deeper assessment draws on multiple domains, including alertness, communication ability, signs of enjoyment, and contextual appropriateness, without relying on a simple checklist. In this phase, we use the Sexual Potential Model4 as a framework to guide nuanced, person-centered evaluation.
Importantly, neither tier treats any single criterion—except for the individual's conscious alertness—as determinative. Rather, it supports a thoughtful, case-by-case deliberation grounded in real-time interactions, not assumptions or projected outcomes. The case is reviewed by a team member who is familiar with the older adult involved, often a psychologist, social worker, or psychiatrist. The SHC collectively makes a recommendation regarding the individual’s consent potential.
How do we assess harm?
The guidelines support staff in reducing the risk of both physical and emotional harm to individuals engaging in sexual activity. Those individuals should also be protected from behavioral restrictions based solely on judgement or bias (eg, same-sex relations, extramarital relationships). With a range of interventions that may reduce the risk of harm, the most appropriate one chosen depends on the individual’s capability of giving sexual consent, the relative risk for the harm involved, and the risks to self or others. According to the reference guide published by the Vancouver Coastal Health Authority,10 the reasonableness of harm depends on the following factors:
- The degree of probability that harm will occur
- The seriousness of the harm
- The availability of less risky alternatives
- The importance of the activity to the person
With these considerations in mind, the guidelines offer several creative examples of risk-mitigating strategies that staff can employ.
How do staff handle sexual behaviors that make staff or other individuals uncomfortable?
This is particularly important for the perpetuation of safe sexual health expression within facilities that are also where people live and work. Discomfort may arise from a range of situations, including uncertainty about an individual’s capacity and consent, exhibitionism, and conflicting cultural norms (eg, a resident with dementia has a girlfriend living in the unit even though he has a wife outside of the facility). Perceptions of problematic sexual behavior can also vary significantly based upon individual beliefs and context. In these moments, comprehensive staff training and open communication are invaluable tools in creating opportunities for productive conversations that focus on older adults’ quality of life while making the situation sustainable for caregivers.
Staff are encouraged to start with the decision tree. Cases are often referred to the SHC, where an interdisciplinary team reviews the following: an objective description of what happened, a consent check, a safety check, and creating supports to improve any areas of concern. Family members may also express discomfort with older adults’ sexuality, but SHC members can address their concerns through education and sharing the process for creating individualized recommendations for their loved one’s sexual health.
The following example illustrates the decision tree in practice: A resident is seen masturbating in the dining room, which is a public space. The first task of the decision tree is to describe the intimate act seen. Then the team evaluates consent, according to the prompts in Tier 1. Given that this act involves only one individual, there are no concerns about consent (answering "Yes" to the decision tree). However, there are concerns about the safety of other individuals in the public area observing the act (answering "No" to the decision tree). Staff may intervene, by redirecting the resident to his private room and closing the door or curtain, where this activity would be appropriate. Staff may assist with safe cleanup afterward. The team is encouraged to debrief after the intervention (eg, proper cleanup strategies, offering materials, such as lubrication, available in his room).
What does debriefing include?
The purpose of debriefing is to review the rationale for each decision that was made during the response; to create or fine-tune a long-term plan for engaging with this particular situation in a sustainable manner; to help identify any “blind spots” or biases; to normalize discussions about older adult sexuality and validate that these situations can be challenging or uncomfortable; and to further align the organization’s culture with its values. The guidelines provide suggested questions that can help direct these debriefing sessions.
Pitfalls and Victories
Developing sexual health guidelines for older adults—particularly those with cognitive impairment—requires more than clinical knowledge and ethical frameworks; it demands collaboration, institutional support, and time investment. Our experience leading such a policy initiative within a large care organization highlighted both the structural challenges and promising victories that can inform future efforts.
One of our most significant obstacles was maintaining continuity of the SHC’s members, which hindered continuous discussion on developing the sexual health guidelines. Staff retention, which represents a continuous problem within the health care setting, has affected the capacity for crucial voices to be part of this movement. In addition, the demands on staff time and schedules made it difficult to plan development meetings.
Support from leadership helped us succeed by allowing us to “get the word out” internally, build awareness, and encourage staff at all levels to see sexual consent and intimacy as integral to person-centered care. Buy-in from management opened doors for deeper conversations and shifted cultural attitudes in subtle but powerful ways. At the same time, the guidelines are used primarily on a case-by-case basis; widespread dissemination hinges on the lengthy institutional review process. We anticipate varying degrees of pushback, shaped by staff schedules, workload, and personal cultural and religious narratives connected to sexuality. Another factor of our success was inviting experts outside of the organization to join the committee, bringing fresh perspectives and ensuring the guidelines were aligned with best practices and innovative research.
Ultimately, our experience affirmed that developing sexual consent guidelines is not just about what ends up on paper. It is about fostering a culture where intimacy, autonomy, and safety are held in balance—where conversations about sexuality in later life are not avoided but welcomed, even when complex.
Future Directions
Training is essential to successful development and implementation of sexual health guidelines, especially as staff need procedural clarity and space to explore their own values and biases. Tailored education sessions that include real-life cases and exploration of the guidelines can build the staff’s confidence in responding compassionately and appropriately to individual needs. Our goal is to create training modules that are specific to each discipline or groupings of disciplines; for example, nursing team members would receive training that focuses on responding to sexual behaviors, as they are often the first to encounter them.
The SHC also aims to provide consultation to team members on long-term care units that express uncertainty about navigating a particular sexual issue. With a formalized process for placing consults in our electronic medical record system, it would be more efficient to review each case, interview the stakeholders involved, and provide individualized recommendations to that team.
While this article outlines the initial steps to create sexual health guidelines in long-term care, ensuring the sustainability of the committee itself is a key component to its long-term success. These efforts may include conducting regular recruitment periods across disciplines, maintaining the discourse on older adult sexual health by contributing to internal and external literature, and garnering the support of the organization’s leadership.
Support from leadership comes in many forms; we have been very fortunate to work with leaders who have promoted conversations about older adult sexual health since the SHC was formed. In the future, committee sustainability would be bolstered by dedicating time to its efforts, holding regular meetings, and providing consultation/liaison services. It will be important for the SHC to demonstrate to leadership that time spent on these ventures is a worthwhile investment. For example, addressing concepts that make staff members feel anxious may help them feel more supported and confident in their roles, thereby improving job satisfaction and potentially reducing turnover. It may also help staff of all disciplines view older adults as human beings with needs for intimacy and autonomy.
Conclusion
The SHC and its sexuality guidelines represent early steps in a movement to provide older adults with comprehensive care that incorporates all aspects of their personhood, including sexual expression. Determining an individual's ability to provide consent remains a nuanced issue that defies simple categorization; although no definitive black-and-white answers may emerge, the guidelines help navigate the intricacies of consent assessment with care and sensitivity. In addition, organizations may use the guidelines and training as a dynamic framework to meet the evolving needs of older adults in their communities. To do so, organizations can become more responsive than reactive to sexual behaviors deemed “problematic” and help proactively create spaces for connection and intimacy with self and others. We invite you to join us in creating opportunities where older adults are fully supported to grow and thrive in all aspects of their humanity.
Key Clinical Summary
- This article describes the development of sexual health guidelines in a long-term care setting to address the often overlooked role of sexuality in the lives of older adults.
- It outlines how one health care organization developed a structured, person-centered framework that supports sexual expression, including a two-tier model for assessing consent and a practical decision tree for staff.
- The guidelines aim to empower staff, promote resident autonomy, and inspire other long-term care facilities to develop their own sexual health guidelines.
Affiliations, Disclosures & Correspondence
Nathalie Huitema, PhD, CSE1 • Rachael F. Arielly, PsyD2 • Sarah J. Rogers, LICSW, CST3
Affiliations:
1 Department of Human Sexuality (HSX), California Institute of Integral Studies, San Francisco, California
2 Department of Medicine, Hebrew SeniorLife, Boston, Massachusetts
3 Sarah Rogers, Malden, Massachusetts
Disclosure: The authors declare no conflicts of interest.
Address correspondence to:
Nathalie Huitema, PhD, CSE
Email: nathalie@drnathaliehuitema.com
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Annals of Long-Term Care or HMP Global, their employees, and affiliates.
References
- World Health Organization. Defining Sexual Health: Report of a Technical Consultation on Sexual Health 28–31 January 2002. World Health Organization; 2006. https://www.worldsexualhealth.net/_files/ugd/793f03_f90b7e05773541739b7c20cf10b63ed7.pdf
- Mahieu L, Dierckx de Casterlé B, Acke J, et al. Nurses’ knowledge and attitudes toward aged sexuality in Flemish nursing homes. Nurs Ethics. 2016;23(6):605-623. doi:10.1177/0969733015580813
- Villar F, Celdrán M, Serrat R, et al. Sexual situations in Spanish long-term care facilities: Which ones cause the most discomfort to staff? Sex Res Soc Policy. 2019;16:446–454. doi:10.1007/s13178-018-0346-9
- Huitema N, Syme M. The sexual consent potential model. Generations Journal. 2022;46(4):1–14. https://generations.asaging.org/sexual-consent-potential-model/
- World Health Organization. Sexual Health, Human Rights and the Law. World Health Organization; 2015. Accessed March 11, 2026. https://www.who.int/publications/i/item/9789241564984
- Koepp R. Sexual health assessment for adults living in long-term care. Center for Mental Health & Aging. March 30, 2022. Accessed May 8, 2025. https://www.mentalhealthandaging.com/sexual-health-assessment-for-adults-in-long-term-care/
- Doll GM. Sexuality in nursing homes: practice and policy. J Gerontol Nurs. 2013;39(7):30-37. doi:10.3928/00989134-20130418-01
- Thys K, Mahieu L, Cavolo A, Hensen C, Dierckx de Casterlé B, Gastmans C. Nurses’ experiences and reactions towards intimacy and sexuality expressions by nursing home residents: a qualitative study. J Clin Nurs. 2019;28(5-6):836-849. doi:10.1111/jocn.14680
- Our mission and heritage. Hebrew SeniorLife. Accessed May 8, 2025. https://www.hebrewseniorlife.org/about-us/our-mission-and-heritage
- Vancouver Coastal Health Authority. Supporting sexual health and intimacy in long-term care homes: a pocket reference guide. May 2023. Accessed May 8, 2025. https://vch.eduhealth.ca/en/permalink/phem4152

